Severe calcific constrictive pericardiectomy operation: ‘Hearts of stone’
Background: Dense constrictive pericarditis, ‘Hearts of stone’ is a rare condition characterized by limitation of myocardium due to a massive fibrosis and calcification of the pericardium. The aim of this study was to research the literature to discuss the surgical intervention and management of densely calcified constrictive pericarditis.
Methods: Over a seven-year period, 19 consecutive patients who underwent pericardiectomy operation for severe constrictive pericarditis reviewed to determine reasons, surgical techniques, mortality and morbidity rates, and improvement of functional capacity. We freed the anterior pericardium from phrenic nerve to phrenic nerve. In two cases, we used a rongeur to break down the dense calcification. The indications for pericardiectomy were tuberculous in 4 cases (21%), idiopathic-fibrous in 11(57.8%), rheumatic in 2(10.5%), uremic in 1(5.2%), and neoplastic in 1(5.2%).
Results: Inpatients mortality ratio was 5.2% in case of isolated severe calcified pericardiectomy. Ascites in 3 patients (15.7%), hepatomegaly in 4 (21%) and peripheral edema in 15 (78.9%) were found on their physical examination. In the 1st postoperative month follow up, dramatically improvement of preoperatively functional capacity were the number of cases in New York Heart Association class IV (worse general condition) moved from 14 to II; in class III from 4 to II; in class II from to I in one case. In our all series, idiopathic-fibrous was the most frequent cause of chronic severe constrictive pericarditis, but the second most common tuberculous pericarditis was increasing overall. Postoperative and neoplastic pericarditis were rare.
Conclusion: The preoperative clinical conditions and functional status at follow-up was improved in all cases. We recommended that the orthopedic surgical instrument, ‘rongeur’, is very useful to cut that totally calcified tissue.
Keywords: Constrictive pericarditis, pericardiectomy, heart failure, calcification
Full Text
Introduction
We reviewed the cases of 19 patients who underwent pericardiectomy operation via median sternotomy for severe constrictive pericarditis, ‘’Hearts of stone’’ between January 2008 and July 2015, to determine causes, treatment options of surgical techniques, mortality and morbidity rates, and improvement of functional capacity. In all patients who has admitted to our clinic for the surgical therapy, cardiac evaluation confirmed constrictive pericarditis. All cases presented with dyspnea on exertion and easy fatigability.
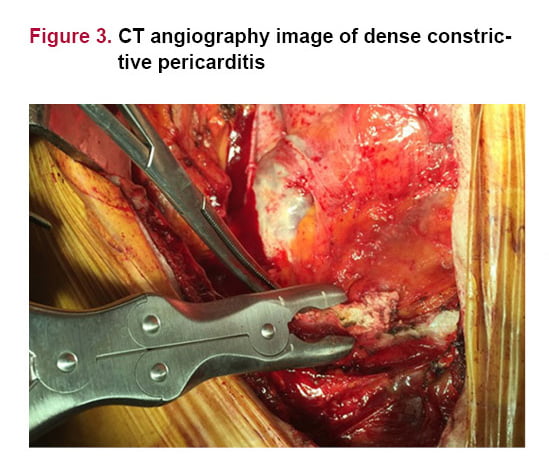
In all cases, the operation was performed thorough median sternotomy. We freed the anterior pericardium from phrenic nerve to phrenic nerve. In two cases, the severe calcified pericardium around both ventricles was so hard to contract because of dense calcified tissue which adhered to the myocardium. Different seizers failed to cut due to severe calcification and adhesion. Therefore, we employed a rongeur to peel off the calcified pericardium gently around the right and left ventricles which performed without the usage of extracorporeal circulation.
The primary outcomes were the risk factors including advanced age, sex, smoking status, hypertension, hyperlipidemia, carotid disease, diabetes mellitus, prior cardiac events, chronic obstructive pulmonary disease, peripheral vascular disease, neurological events, HbA1c levels, and serum creatinine levels. The secondary outcomes were of preoperative New York Heart Association (NYHA) heart failure functional class and left ventricular ejection fraction. Other outcome measures were perioperative death (in hospital) and intensive care unit vital follow up. In all calculations and statistical analyses, “Statistical Package for Social Sciences” (SPSS-Chicago, IL, USA) 16 and Software Excel (Microsoft-USA) programs were used. The statistical results are presented as mean values.
Results
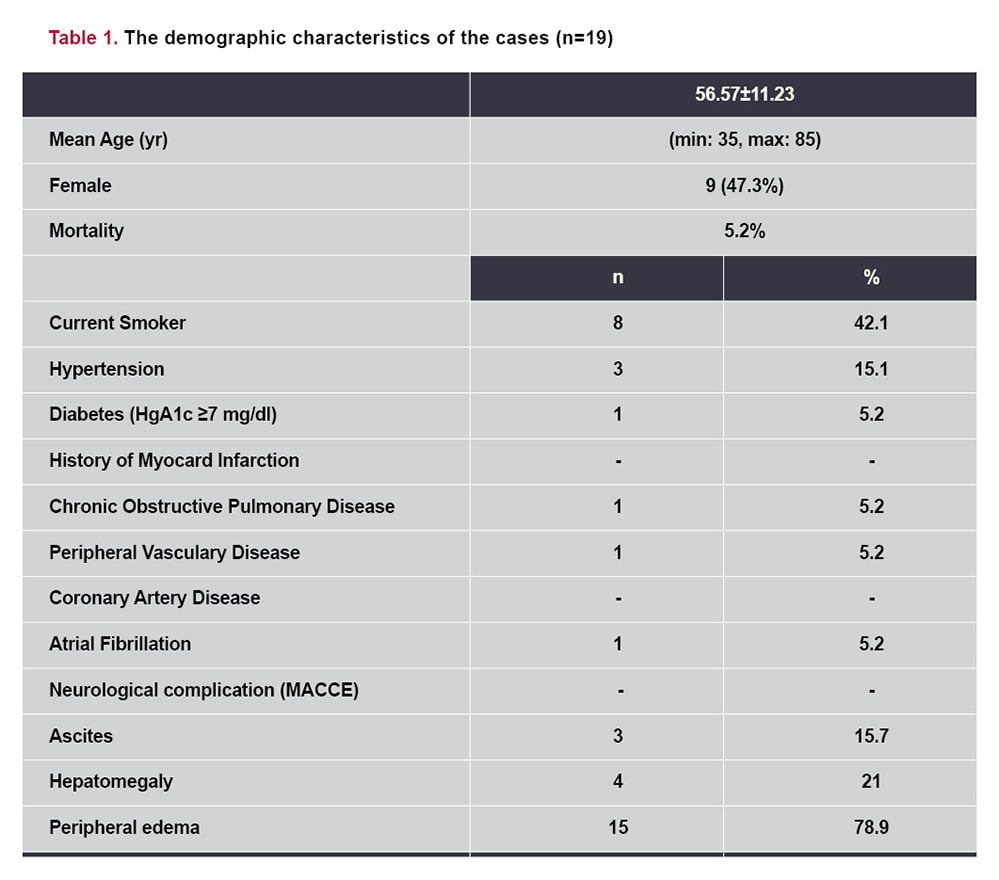
During the 7-year period between January 2008 and July 2015, we performed pericardiectomy operation thorough median sternotomy on 19 cases with a diagnosis of constrictive pericarditis. The cases consisting of 9 female (47.3%), 10 male (52.2%) were found. 19 cases with an average age of 56.57 years (min: 35, max: 85) (11.23 SD) have been observed.
Ascites in 3 patients (15.7%), hepatomegaly in 4 (21%) and peripheral edema in 15 (78.9%) were found on their physical examination. The cases operated on within 2 months after the onset of symptoms. Laboratory results found hyponatremia, hypoproteinemia and hypoalbuminemia in all cases. The mid-term survival was satisfactory. There was no any neurological complication (postoperative major adverse cardiovascular and cerebral event (MACCE) during pericardiectomy operation. Comorbidities related to the patient group were the diabetes mellitus in 1 case (5.2%) (Insulin de-pendent-HbA1c median ratio 7.78) and the hypertension in 3 cases (15.1%). There was 1 case (5.2%) with atrial fibrillation. None of the cases had concomitant coronary artery disease. Chronic Obstructive Pulmonary Disease was observed in 1 case (5.2%). Alcohol use was not found. Smoking was observed in 8 patients (42.1%). Preoperatively, four of the 19 patients (21%) had needed pericardiocentesis. These patients had taken diure-tics and digitalis at optimal doses for heart failure.

Discussion
Hirai et al.[8] detected that using an ‘Ultrasonic Scalpel’ is a useful method for treatment of chronic constrictive pericarditis, and advocate the use of the Ultrasonic Scalpel for a safe and easy pericardiectomy. The scalpel, curette, and rongeur are used for gouging out bone in neurosurgery and orthopedic surgery.[5] Regarding the surgical treatment of severely calcific constrictive pericarditis, a rongeur can also be used in dissection of severely calcified pericardium. Another difficulty in ca-ses, we used rongeur previously. We offer that a rongeur is very useful for peeling off the densely calcified pericardium. Phrenic nerve-during pericardiectomy must be protected. Global left ventricular regional wall motion should be observed carefully during the surgery.
Also, experienced surgical approach is essential for successful severe calcific pericardiectomy. In order to maintain hemodynamic stability; careful manipulation of the heart and pericardial incision, intra-aortic balloon pump and pacing wires preparation, pharmacological interventions, and anesthesia monitoring are very important. Inotropic agents are essential to maintain cardiac output during the manipulations. In addition, the availability of heart-lung machine and perfusionist are necessary for temporary support. The follow-up is required with a great experience. Fluid and electrolyte balance must be protected during the operation and intensive care unit.
Conclusion
References
- Goel PK, Moorthy N. Tubercular chronic calcific constrictive pericarditis. Heart Views 2011;12(1):40-1.
- Yetkin U, Kestelli M, Yilik L, et al. Recent surgical experience in chronic constrictive pericarditis. Tex Heart Inst J 2003;30(1):27-30.
- Liu S, Ma C, Ren W, et al. Regional left atrial function differentiation in patients with constrictive pericarditis and restrictive cardiomyopathy: a study using speckle tracking echocardiography. Int J Cardiovasc Imaging 2015(7):6.
- Seidler S, Lebowitz D, Müller H. Chronic constrictive pericarditis. Rev Med Suisse 2015;11(476):1166, 8-71.
- Budjan J, Haghi D, Henzler T, et al. Myocardial herniation in constrictive pericarditis mimicking arrhythmogenic right ventricular cardiomyopathy. Eur Heart J 2015(6):18.
- Negishi K, Popovic ZB, Negishi T, et al. Pericardiectomy is Associated with Improvement in Longitudinal Displacement of Left Ventricular Free Wall Due to Increased Counterclockwise Septal-to-Lateral Rotational Displacement. J Am Soc Echocardiogr 2015(6):1.S0894-7317(15)00383-1.
- Ota T, Mizutani T. Microscopic anterior clinoidectomy with micro-rongeurs for a superior projecting paraclinoid internal carotid artery aneurysm: a technical note. Br J Neurosurg 2013;27(4):540-2.
- Hirai S, Hamanaka Y, Mitsui N, et al. Surgical treatment of chronic constrictive pericarditis using an ultrasonic scalpel. Ann Thorac Cardiovasc Surg 2005;11(3):204-7.
- DeValeria PA, Baumgartner WA, Casale AS, et al. Current indications, risks, and outcome after pericardiectomy. Ann Thorac Surg 1991;52(2):219–24.
- Girardi LN, Ginsberg RJ, Burt ME. Pericardiocentesis and intrapericardial sclerosis: effective therapy for malignant pericardial effusions. Ann Thorac Surg 1997;64:1422–8.
- Panchal P, Adams E, Hsieh A. Calcific constructive pericarditis: a rare complication of CREST syndrome. Arthritis Rheum 1996;39(2):347–50.
- Watanabe A, Hara Y, Hamada M, Kodama K, Shigematsu Y, Sakuragi S, et al. A case of effusive-constructive pericarditis: an efficacy of GD-DTPA enhanced magnetic resonance imaging to detect a pericardial thickening. Magnetic Resonans Imaging 1998;16(3):347–50.
- Lominadze Z, Kia L, Shah S, et al. Constrictive Pericarditis as a Cause of Refractory Ascites. ACG Case Rep J 2015;10;2(3):175-7.
- Tsang MY, Choi JO, Borlaug BA, et al. Low-Flow, Low-Gradient Severe Aortic Stenosis in the Setting of Constrictive Pericarditis: Clinical Characteristics, Echocardiographic Features, and Outcomes. Circ Cardiovasc Imaging 2015;8(7):e002812.
- Choi JH, Uhm JS, Lee SE, et al. Constrictive Pericarditis Long after a Gunshot Wound. Korean Circ J 2015;45(4):333-6.35.